I have no position on the effectiveness of any drug. But the censorship surrounding HCQ is very disturbing. Seven years ago, Dr. Fauci supported experimental medicines to fight a deadly novel coronavirus.
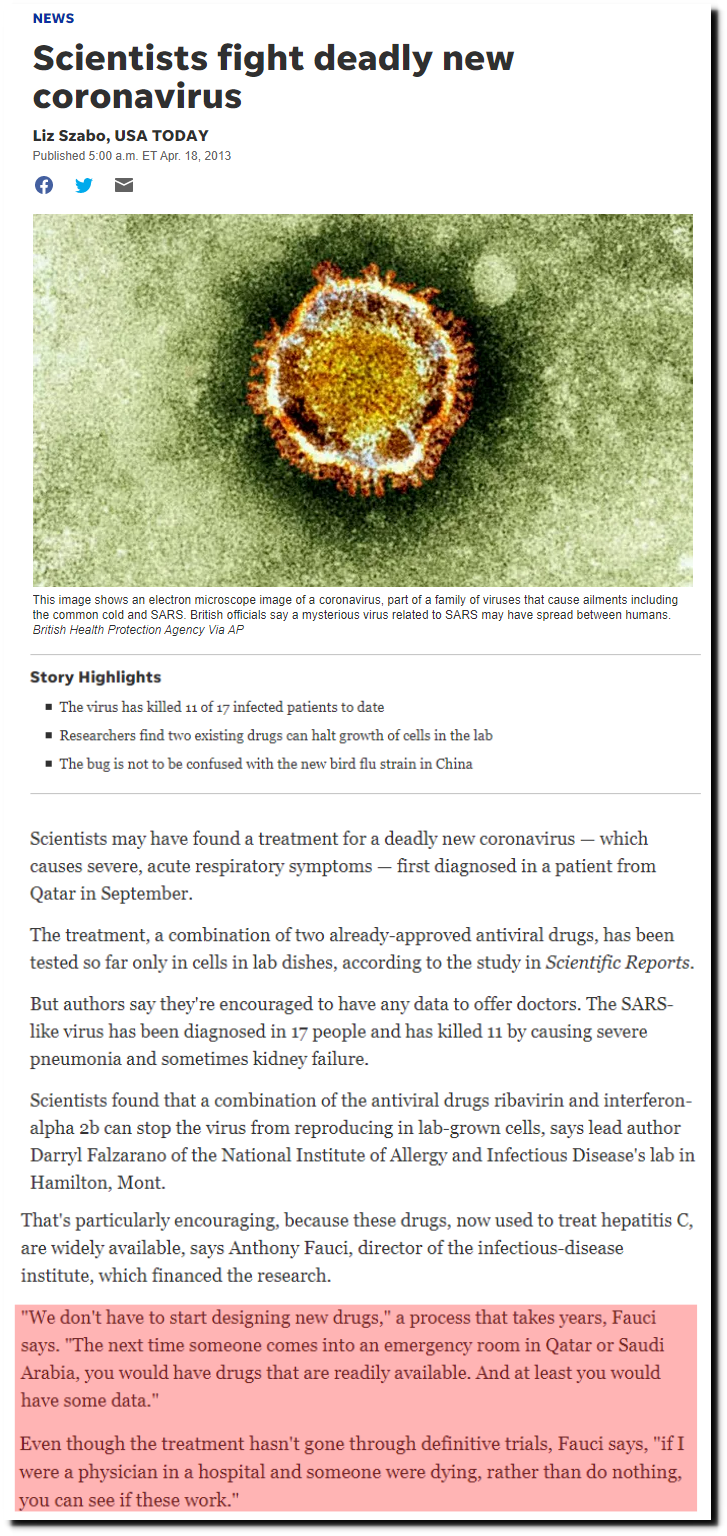
Scientists fight deadly new coronavirus
Fifteen years ago, Fauci’s NIH said HCQ was a potent inhibitor or coronaviruses.
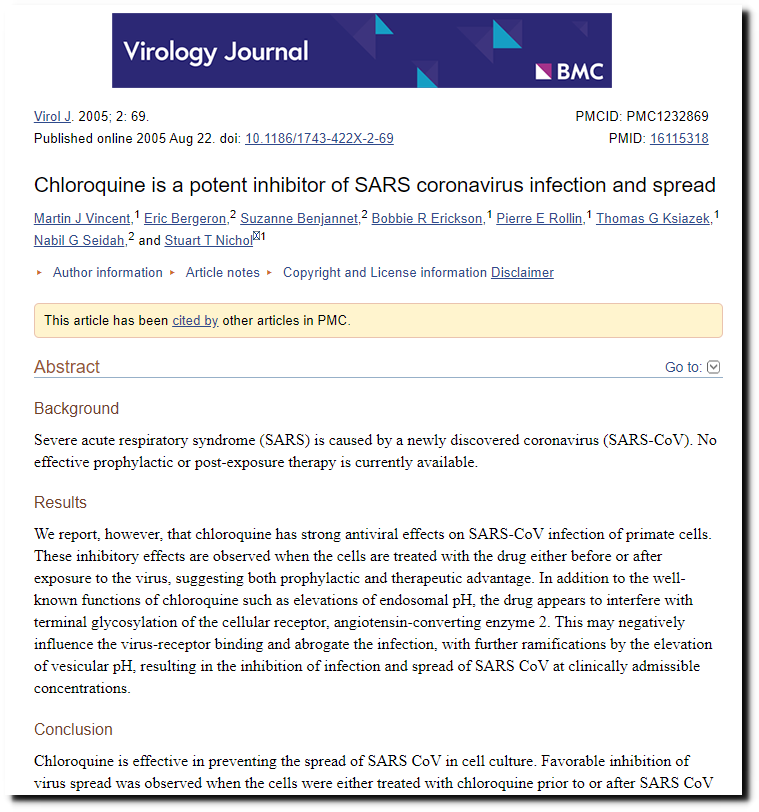
Chloroquine is a potent inhibitor of SARS coronavirus infection and spread
Now Fauci is leading the charge to discredit and censor discussion about HCQ treating coronaviruses. Including that from the world’s leading infectious disease expert.
He Was a Science Star. Then He Promoted a Questionable Cure for Covid-19. – The New York Times
The President, his son and even Madonna have been censored by Twitter, Facebook and Instagram for saying the same thing which Fauci’s NIH said fifteen years ago. The Guardian uses the term “right wing” to cancel people, in exactly the same way which the term “Jew” was used to cancel people in the 1930s.
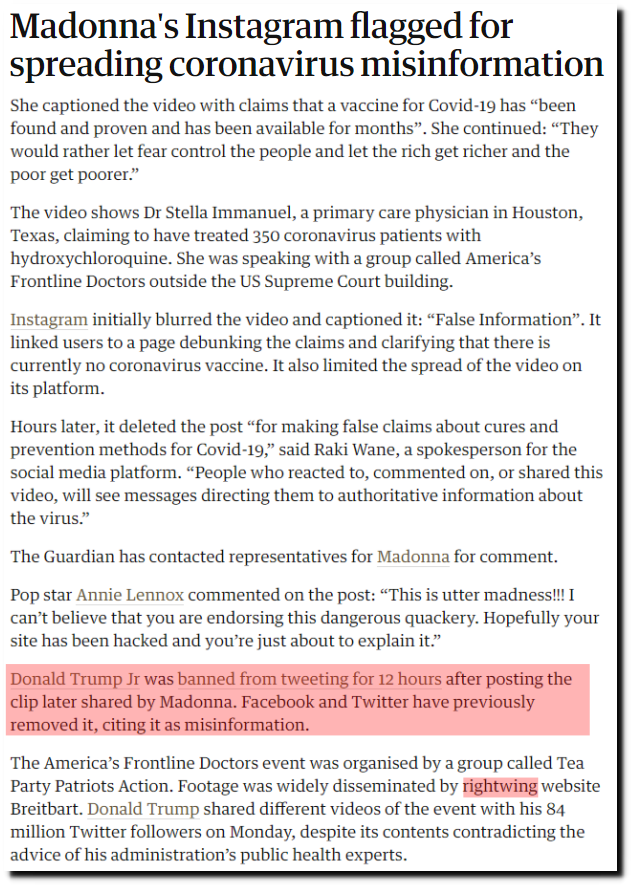
Madonna’s Instagram flagged for spreading coronavirus misinformation | Music | The Guardian
This paper from the censored group of doctors provides pretty strong arguments that HCQ is both safe and effective.
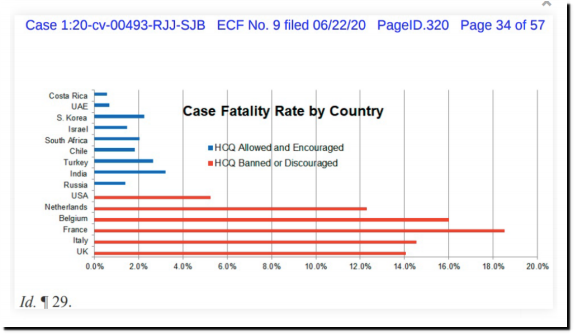
And another.
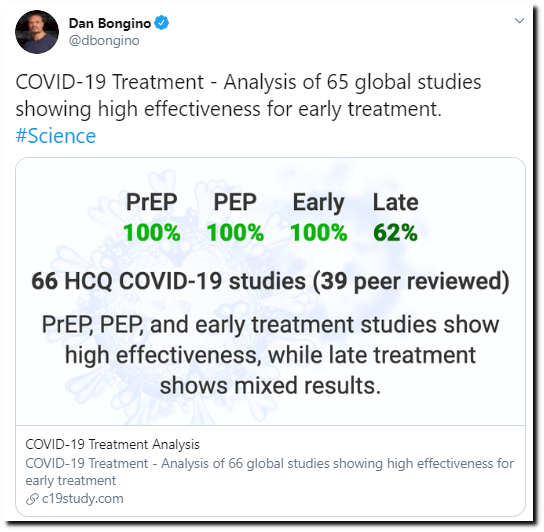
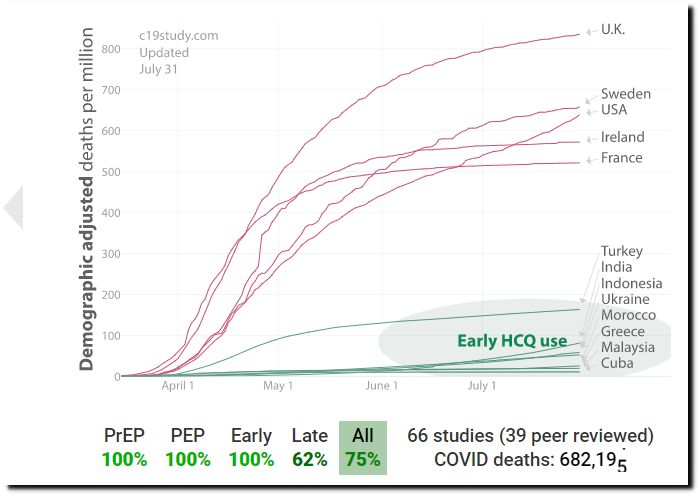
COVID-19 Treatment – Analysis of 66 global studies showing high effectiveness for early treatment
Trump Defends Pro-Hydroxychloroquine Video After Social Media Ban
So why is Fauci engaged in this cover up and censorship? One possible explanation is this FDA rule. An emergency medical medicines/vaccines authorization is not possible if there are approved alternatives.